Twenty years of breast cancer in Iran: downstaging without a formal screening program
Abstract
Background: Breast cancer (BC) is the most common malignancy among Iranian women. Although the relative incidence of BC is low, the cause-specific mortality is much higher than developed countries. The present study surveyed the overall trend of BC in Tehran.
Patients and methods: All breast pathologic records were studied in five major hospitals in Tehran during three phases (1: 1985–1995; 2: 1996–2000; and 3: 2001–2005). Malignant cases were classified according to the tumor–node–metastasis classification. Data were compared across the study.
Results: Of 9050 medical records from male and female patients with ‘breast disease’, 2946 females with BC were included. A significant increase in the diagnosis of palpable early BCs (stage II increased, stage III decreased) was observed between phases 1 and 2. A relative increases in stages 0 and I were noted between phases 3 and 2. Nevertheless, 76.8% of cases were T2 or higher and 65.3% had positive lymph nodes in the last phase. The proportion of patients with stage IIIb was increased in phase 3, despite the reduction in phase 2.
Conclusions: Despite the relative improvement in the status of BC patients, the vast majority are diagnosed in advanced stages. Specific screening measures should be implemented in Iran.
Keywords: breast cancer; Iran; staging; trend
Authors: Iraj Harirchi, Shadi Kolahdoozan, Mojgan Karbakhsh-Davari, N.Chegini1, Sakineh Moaid Mohseni, Ali Montazeri, Amir Javad Momtahen1, Amir Kashefi1, Mandana Ebrahimi
https://doi.org/10.1093/annonc/mdq303
Journal: Annals of Oncology | Volume 22, Issue 1, January 2011, Pages 93-97 (Link)
Introduction
Cancer is the second leading cause of death worldwide [1, 2], and the global burden has increased >two-fold over the past 30 years [2]. Breast cancer (BC) is the most frequent cancer (23% of all cancers) [3] and the most fatal form of malignancy among women [2, 4], accounting for 16% of cancer deaths [1]. Therefore, BC remains a major health problem worldwide.
There are some differences in the reported incidence rates of BC throughout the world as follows: highest in North America [age-standardized rate (ASR): 123.6 per 100 000] [5] and Western Europe (ASR: 84.6 per 100 000) [3], intermediate in the Mediterranean and South American countries (ASR: 46 per 100 000) [3], and lowest in Southeast (ASR: 25.5 per 100 000) [3, 6] and South Central Asia (ASR: 21.8 per 100 000) [3]. Although the prevalence of BC in Asia is low, the cause-specific mortality and the increment in incidence in most Asian countries are much higher than in Western countries [7], which can be due to increased life expectancy and changes in reproductive and behavioral patterns associated with a heightened BC risk [2].
In Iran, BC is ranked first among malignancies among women [8, 9], comprising 24.4% of all neoplasms [10] with a crude incidence rate of 17.81 [9] and an ASR of 23.65 [9] in the year of 2006. However, studies [11., 12., 13., 14.] specifically describing the clinicopathologic features, stages, and age distributions of BC in Iran are limited; thus, it is difficult to predict the present and future patterns of BC and carry out the most appropriate preventive and therapeutic measures to decrease the burden of the disease in Iran [12]. In addition, concerning the high mortality rate of BC in developing countries [7] and the increasing incidence, an epidemiologic evaluation with demographic trend analysis focusing on the recent shift in the age of presentation should be considered for primary and secondary prevention of BC [14, 15].
The present longitudinal survey studied the overall spectrum, burden, and characteristics of female BC in Tehran, Iran. Since the results of this study can provide basic information about the early diagnosis, treatment, and management of BC, it may contribute to improve the outcomes of such patients.
The current study is the largest survey on BC in Iran to date. Therefore, by retrieving this unique long-term data (20 years), we may be able to assess and compare several aspects of BC, particularly the clinical and epidemiologic changes over a long period of time in Tehran, Iran.
patients and methods
Since 1995, the Iranian Center for Breast Cancer has implemented a collaborative multicenter cross-sectional study on BC from 1985 to 2005 in Tehran metropolitan area. Because Iran’s cancer registry center had not been established at the beginning of the current study, the study was carried out in five general district and teaching hospitals (Imam Khomeini, Sina, Dr. Shariati, Shohaday-e Tajrish, and Shahid Mustafa Khomeini) to gather all breast pathologic records.
All medical records and reports of pathologic specimens from patients with the diagnosis of ‘breast disease’ were reviewed in a retrospective study from 1985 to 1995. All female BC documents were surveyed to promote a comparison and demonstrate the trend. The following information, including date of birth, gender, type of disease according to the International Classification of Diseases, 10th revision (ICD-10) and International Classification of Diseases for Oncology (ICD-O) classification guidelines, pathologic staging for malignant tumors based on the American Joint Committee on Cancer classification, fifth edition [16], tumor size (in centimeter), lymph node involvement, type of surgery carried out, and side and location of the tumor, were obtained by trained practitioners based on a confirmed questionnaire. It should be mentioned that TNM (tumor–node–metastasis), ICD-O, and ICD-10 were not included in the preliminary pathology reports, especially in the first 10 years, so all reports were reclassified by the same practitioners. The study was continued as a prospective study from 1995 to 2005 based on the same guidelines. Although there is a newer version of the TNM staging system, we used the fifth edition to be able to extract homogeneous data for analysis and comparison to initial experiences [11, 12, 14].
To improve the sample accuracy, we did not study cases from referral centers, such as the Iranian Cancer Institute. We also were unable to stage the cancer clinically due to a lack of information on metastasis status. The results of last part of the study (2001–2005, phase 3) were extracted and compared with previous data (1985–1995, phase 1 and 1996–2000, phase 2). Eventually, we were able to demonstrate characteristic changes in BC of residents of Tehran during the 20 years. The study was approved by the Tehran University of Medical Sciences Review Board. SPSS, version 17 (SPSS Inc., Chicago, IL) was used for statistical analysis and an α = 0.05 was considered as the level of statistical significance.
results
From 1985 to 2005, 9050 medical records labeled as breast disease in both genders were reviewed. Of the 9050 medical records, 2946 female patients had a diagnosis of BC and were included in the study. Primary BC in women was the main focus of the present study. Detailed characteristics of BC in this surveys (phases 1, 2, and 3) are demonstrated in Table 1.
Table 1. Characteristics of women with breast cancer in a multicenter study in Tehran, Iran [percents are calculated according to valid (nonmissing) cases]
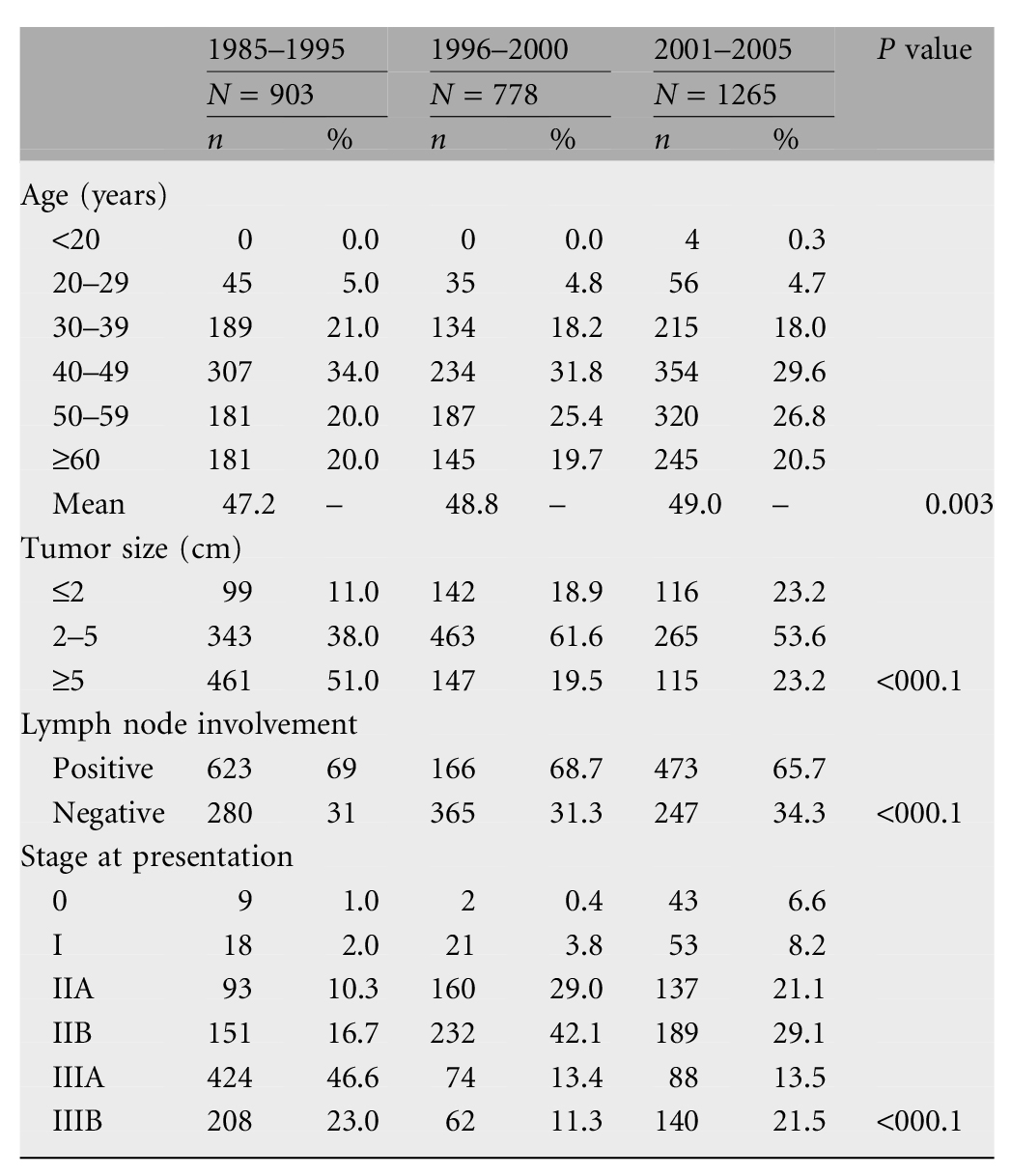
An increasing trend in the diagnosis of early BC (stages 0 and I) was observed; specifically, 3.0%, 4.2%, and 14.8% of BC cases in phases 1, 2, and 3 were stages 0 and I, respectively (P < 0.001). Also, the total in situ lesions increased from 0.1% and 0.3% in phases 1 and 2, respectively, to 6.3% in phase 3 (P = 0.004). The proportion of tumors <2 cm in diameter increased during the survey (phase 1, 11.0%; phase 2, 18.9%; and phase 3, 23.2%; P < 000.1).
Another significant finding was the dramatic increase in the proportion of stage II BC (IIA and IIB); 27.0% and 71.1% of cases were stage IIA and IIB in phases 1 and 2, respectively, while the number of cases of advanced breast cancer (stages IIIA and IIIB) decreased from 69.6% in phase 1 to 24.7% in phase 2 of the survey. Figure 1 shows the changes in trend with respect to disease stage at diagnosis during the study period. Likewise, the frequency of tumors 2–5 cm in size increased (38.0%–61.6%) between phases 1 and 2, but the frequency of tumors >5 cm in size decreased (51.0%–19.5%) from phase 1 to phase 2 of the study (P < 0.001).
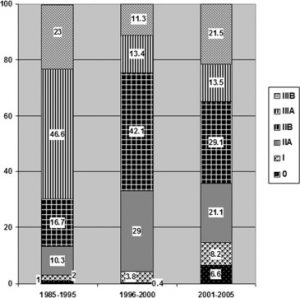
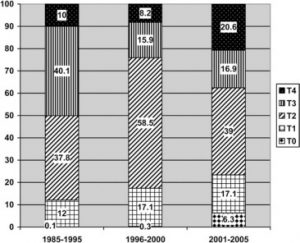
Some important and unexpected issues were observed during the phase 2–3 analysis, as follows: the increment of stage IIIB increased from 11.3% to 21.5% (P < 0.001), the increase in frequency of cases with T4 at presentation increased (8.2% to 20.6%, P = 0.009), and the increase in proportion of tumors >5 cm from 19.5% to 23.2% (P = 0.6).
Considering the local extension of tumors, ∼6.3% of all malignant lesions were T0, 17.1% were T1, 39.0% were T2, 16.9% were T3, and 20.6% were T4 at presentation from 2001 to 2005 (Figure 2). Our data show that stage IIIA cancer was the most prevalent stage (46.6%) in phase 1, while stage IIB was dominant in phases 2 (42.1%) and 3 (29.1%). The frequencies of tumors with sizes >2 cm were 89.0%, 81.1%, and 76.8% in phases 1, 2, and 3, respectively. Although we saw a relative reduction in lymph node involvement during the survey (phase 1, 69.0%; phase 2, 68.7%; and phase 3, 65.7%), the high rate of lymph node involvement is important.
For all malignant lesions, breast-conserving surgery (BCS) was carried out in 2.0%, 4.3%, and 6.0% of patients in phases 1, 2, and 3, respectively (Fisher’s exact test = 0.4), representing a minor increase across 20 years of study. All the remaining patients underwent various types of mastectomies.
Most conditions were diagnosed in women with a mean age (SD) of 47.0 (12.2), 48.8 (12.6), and 49.0 (12.6) years in phases 1, 2, and 3, respectively (P = 0.002; age range 15–90 years). Therefore, BC mainly affects patients in the fifth decade of life [n = 895 (30.4%)], followed by the sixth decade [n = 688 (23.4%)] and seventh plus decade [n = 571 (19.4%)].
The most common type of breast malignancy was invasive ductal carcinoma (89.2% of patients). Malignant lesions were most often located in the upper outer quadrant of the affected breast (45.7%). The distribution of breast involvement was 50.1% in the left breast, 49.7% in the right breast, and 0.2% bilateral.
Discussion
BC is the most prevalent malignancy among women [3]. According to a report of the Ministry of Health and Medical Education in Iran [10], BC has become the most common primary female cancer in Iranian women. Although the incidence of BC is still low compared with Western countries (Iran, 23.65 per 100 000 and United States, 140.8 per 100 000 Caucasian women), the number of patients with newly diagnosed breast cancer increased during the course of the current survey.
During recent decades, the incidence of female BC increased worldwide. Several studies [17, 18] have reported locally advanced BC as the main presentation at first examination in developing countries, such as Iran [14, 15], a phenomenon that was noted in the current study as well. According to our survey, there was a dramatic increase in the proportion of stage II BC cases from phase 1 to 2 and a decrease in the advanced BC cases from phase 1 to 2. In addition, there was a relative increase in the frequency of tumors 2–5 cm in size and a relative decrease in tumors >5 cm in size between phases 1 and 2 of the study. Thus, we had improvement in the diagnosis of palpable breast masses, especially from phase 1 to 2. These findings can be explained by an overall improvement in the level of health in Iran during the past 20 years. These improvements include an increase in the Human Development Index, Life Expectancy at Birth and Adult Literacy Rate, and an increase in the number of physicians and surgeons available (a detailed description is given elsewhere [14, 19]).
Another important finding of the current study was a statistically significant increase trend in the detection of early stage BC in phase 3 compared with phases 1 and 2 (Table 1). An increase in the proportion of tumors <2 cm in size was noted during the course of the survey. Although the BC detection methods were not intensely investigated in our study, we know that masses are nonpalpable in the majority of stage 0 cancers and the relative majority of stage I cancer or tumors <2 cm (early stages) in size, so the plurality proportion of these subgroup patients in phase 3 demonstrates that the most likely these masses are detected by mammography screening or perhaps clinical examination and/or self-examination. The increased rate of detection of early BC may be raised owing to of the increased awareness on the part of Iranian women with respect to the types of BC screening, especially mammography, increased medical advice, and increased availability mammography devices. It is important to note that regular screening mammography is not available through BC screening programs in Iran, so opportunistic screening mammography is increased due to the above-mentioned issues.
In general, a downstaging trend in BC has occurred in Iran, despite the lack of formal screening programs. This may be due to an increasing awareness among Iranian women about the warning signs of BC, enhanced available health services, and an improvement in socioeconomic status [14].
The results of our survey yielded some major changes and unexpected evidence regarding the predominance of cases at advanced stages between phases 2 and 3; specifically, the increment in the proportion of stage T4 tumors, an increasing detection in tumors >5 cm in size, and multiplication of patients with stage IIIB disease. In fact, despite all significant or relative improvements which occurred continuously in the diagnostic facilities in all three phases [14], the diagnosis of locally advanced tumors increased between phases 2 and 3. Of these cases, most of them were patients in stage T4 with skin involvement. Due to the clinical condition and tumor size at the time of diagnosis, it appears that tumors are palpable and could be detected and treated earlier if physician’s examination, suitable diagnosis, and treatment plans are established in a timely manner. In contrast to an improvement in all social indicators in the community health sector in phase 3 compared with phase 2 (such as the Human Development Index) [19], we encountered a group of patients who had postponed their examination or medical diagnostic procedures after necessary warnings about their medical situation. However, we did not evaluate the causes of delay in diagnosis and treatment in this study. The issue may be due to increased out-of-pocket costs in medical payments; therefore, the Parliament of Iran passed a bill which mandates the governor to pay all hospitalization costs for people without insurance coverage in public hospitals after 2003. Indeed, all rural people were covered by public insurance beginning in 2005.
In the last phase of the study, the frequencies of referred and diagnosed patients in stages II and III were 50.2% and 35.0%, respectively. If the metastatic status of patients was considered, some patients would be restaged in the higher stages. Since the majority of patients with higher stages of BC would be referred to diagnostic and treatment centers [15] and would have a poorer survival outcome in developing countries compared with Western nations [4, 20, 21], early detection should be emphasized in such countries [21]. Moreover, some baseline characteristics of BC, such as age at the time of presentation, are different between several nations that require unique, specific, simple, cost-effective, evidence-based, and culturally appropriate screening programs based on their needs and the priorities of health care system [15, 22]. This subject is an important topic that policy makers should consider as crucial for health care policies and address it through theoretic and empirical analyses. Also, it seems an attempt to set up more efficient and simpler approaches than mammography have revealed more health benefits in Iran [15].
Other important matters include the high rate of patients with lymph node involvement at the first visit, despite the relative reduction in lymph node involvement from 69.0% and 68.7% in phases 1 and 2, respectively, to 65.7% in phase 3, thus more advanced disease at the time of diagnosis and a worse outcome in Iranian women.
It should be mentioned that in spite of the slight increase in proportion of women receiving BCS across the 3 phases, the overall rate of BCS performance in Iran is still low [23]. The most common reasons include advanced disease at the first visit of patients and diagnosis time, less familiarity of the surgeon with BCS, and insufficiency of experience with the BCS technique among oncologists surgeons [23].
In the present study, the age distribution analysis of BC showed the highest incidence among women 40–49 years of age [mean age (±SD): 48.4 years (±12.5)], followed by the sixth and seventh plus decades (Figure 3). This age distribution differs from that of Western countries [24] but is similar to developing nations [25]. This finding indicates that the peak incidence of age for BC is ∼10 years earlier in Iran, which is consistent with previous studies [26].
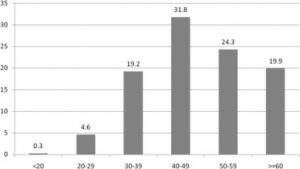
Although Iran is one of the countries with a high rate of young people and the majority of population (86.1%) is <50 years of age [27], even after age-adjusted analysis (based on female age distribution in Tehran, derived from 2005 census), the observed number of patients in the 40- to 49-year-old age group was significantly higher than expected (P < 0.001), so the finding was not due to the younger age of the population. It would be worthwhile to mention that best choice of BC screening and treatment should be age group oriented, especially in Iranian patients [15] because mammographic screening results in women 40–49 years of age are worse than those in women >50 years of age due to dense breasts [28]. Furthermore, with respect to the mean age of menopause [50.4 (±4.3) years] [29] in Iranian women, it appears that BC affects the majority of patients in the premenopause age throughout the survey. This can be an important clue to the reduction in accuracy, effectiveness, and power of mammography as a BC screening tool in younger Iranian women because it has less sensitivity in the premenopause patients due to high density of breast tissue and also difficulty in evaluation of breast micro-classification by mammograms in these ages [30].
In summary, since BC risk factors in premenopausal women [26] are diverse from postmenopausal females, we need to pay more attention in choosing appropriate screening tools.
The average age at the time of diagnosis of BC gradually increased in a slight but meaningful trend during the survey. This finding can be attributed to the improvement in life expectancy and increasing average age of women with BC and increasing awareness of older women with respect to opportunistic screening, which causes higher enrollment of the older subjects in the BC screening programs.
Limitations
This survey gathered aggregate (hospital level) information about BC because Iran’s cancer registry center was not established at the inception of the study, although as an advantage of this study, we excluded referral centers, such as clinics of the Iranian Cancer Institute to improve generalizability of the results.
Lack of data access for estimation of clinical staging and tumors metastasis was another limitation of this study. In addition, we did not review menopausal status of our patients specifically, and absence of information on estrogen or progesterone receptors of patients in our survey is another notable issue.
Furthermore, it is clear that additional data on the evolution of demographic, anthropometric, and nutritional characteristics to parallel this survey would enrich the value of results; however, our data regarding demographic characteristics are scarce and no other data on anthropometric and nutritional characteristics are available to parallel with our observation.
In summary, regardless the data that have emphasized reduction in trend of BC stages over 20 years in Iran, the BC stages of Iranian female patients at the time of diagnosis is higher than developed nations, so health policy makers should consider it as crucial for health policies. It also seems that a major subset of patients are neglected at early palpable stages of BC that could be diagnosed by a self-examination training program or suitable and available screening tools, so we should pay more attention to BC screening programs and acquire appropriate plans according to specific characteristics of female Iranian patients with BC.
References
- The Top 10 Causes of Death in 2004, Fact Sheet of WHO Report, World Health Organization (2008)
Google Scholar - World Cancer Report 2008. WHO.
http://www.iarc.fr/en/publications/pdfsonline/wcr/2008/index.php (2 January 2010, date last accessed)
Google Scholar - D.M. Parkin, F. Bray, J. Ferlay, et al.
Global cancer statistics, 2002
CA Cancer J Clin, 55 (2005), pp. 74-108
CrossRef View Record in Scopus Google Scholar - B.O. Anderson, R. Jakesz
Breast cancer issues in developing countries: an overview of the Breast Health Global Initiative
World J Surg, 32 (2008), pp. 2578-2585
CrossRef View Record in Scopus Google Scholar - A. Jemal, R. Siegel, E. Ward, et al.
Cancer statistics, 2009
CA Cancer J Clin, 59 (2009), pp. 225-249
CrossRef View Record in Scopus Google Scholar - D.M. Parkin, S.L. Whelan, J. Ferlay, et al.
Cancer Incidence in Five Continents, Volume VIII. IARC Scientific Publication No. 155
International Agency for Research on Cancer, Lyon, France (2002)
Google Scholar - K. Shibuya, C.D. Mathers, C. Boschi-Pinto, et al.
Global and regional estimates of cancer mortality and incidence by site: II. Results for the global burden of disease 2000
BMC Cancer, 2 (2002), p. 37
View Record in Scopus Google Scholar - A. Sadjadi, M. Nouraie, M.A. Mohagheghi, et al.
Cancer occurrence in Iran in 2002, an international perspective
Asian Pac J Cancer Prev, 6 (2005), pp. 359-363
Google Scholar - S.M. Mousavi, M.M. Gouya, R. Ramazani, et al.
Cancer incidence and mortality in Iran
Ann Oncol, 20 (2009), pp. 556-563
Article Download PDF View Record in Scopus Google Scholar - M. Goya
Iranian Annual Cancer Registration Report 2005/2006
Ministry of Health and Medical Education, Health Deputy, Center for Disease Control and Prevention (In Persian). Tehran, Iran (2007)
Google Scholar - I. Harirchi, M. Ebrahimi, N. Zamani, et al.
Breast cancer in Iran: a review of 903 case records
Public Health, 114 (2000), pp. 143-145
Article Download PDF CrossRef View Record in Scopus Google Scholar - I. Harirchi, M. Karbakhsh, A. Kashefi, et al.
Breast cancer in Iran: results of a multi-center study
Asian Pac J Cancer Prev, 5 (2004), pp. 24-27
View Record in Scopus Google Scholar - A. Rezaianzadeh, J. Peacock, D. Reidpath, et al.
Survival analysis of 1148 women diagnosed with breast cancer in Southern Iran
BMC Cancer, 9 (2009), p. 168
View Record in Scopus Google Scholar - I. Harirchi, M. Karbakhsh, A. Montazeri, et al.
Decreasing trend of tumor size and downstaging in breast cancer in Iran: results of a 15-year study
Eur J Cancer Prev, 19 (2010), pp. 126-130
View Record in Scopus Google Scholar - S.M. Mousavi, I. Harirchi, M. Ebrahimi, et al.
Screening for breast cancer in Iran: a challenge for health policy makers
Breast J, 14 (2008), pp. 605-606
CrossRef View Record in Scopus Google Scholar - I.D. Fleming, J.S. Cooper, D.E. Henson, et al.
American Joint Committee on Cancer: AJCC Cancer Staging Manual
(5th edition), Lippincott-Raven, Philadelphia, PA (1997)
Google Scholar - G. Agarwal, P. Ramakant, E.R. Sanchez Forgach, et al.
Breast cancer care in developing countries
World J Surg, 33 (2009), pp. 2069-2076
CrossRef View Record in Scopus Google Scholar - C.H. Yip
Breast cancer in Asia
Methods Mol Biol, 471 (2009), pp. 51-64
CrossRef View Record in Scopus Google Scholar - Human Development Report 2007/2008.
http://hdr.undp.org/en/reports/global/hdr2007-2008/ (1 January 2010, date last accessed)
Google Scholar - B.O. Anderson, R. Shyyan, A. Eniu, et al.
Breast cancer in limited-resource countries: an overview of the Breast Health Global Initiative
2005 guidelines, Breast J, 12 (Suppl 1) (2006), pp. S3-S15
View Record in Scopus Google Scholar - R.A. Smith, M. Caleffi, U.S. Albert, et al.
Breast cancer in limited-resource countries: early detection and access to care
Breast J, 12 (Suppl 1) (2006), pp. S16-S26
View Record in Scopus Google Scholar - B.O. Anderson, S. Braun, S. Lim, et al.
Early detection of breast cancer in countries with limited resources
Breast J, 9 (Suppl 2) (2003), pp. S51-S59
CrossRef View Record in Scopus Google Scholar - M. Najafi, M. Ebrahimi, A. Kaviani, et al.
Breast conserving surgery versus mastectomy: cancer practice by general surgeons in Iran
BMC Cancer, 5 (2005), p. 35
View Record in Scopus Google Scholar - C. Smigal, A. Jemal, E. Ward, et al.
Trends in breast cancer by race and ethnicity: update 2006
CA Cancer J Clin, 56 (2006), pp. 168-183
CrossRef View Record in Scopus Google Scholar - S. Rodriguez-Cuevas, C.G. Macias, D. Franceschi, et al.
Breast carcinoma presents a decade earlier in Mexican women than in women in the United States or European countries
Cancer, 91 (2001), pp. 863-868
View Record in Scopus Google Scholar - A. Montazeri, M. Ebrahimi, N. Mehrdad, et al.
Delayed presentation in breast cancer: a study in Iranian women
BMC Womens Health, 3 (2003), p. 4
View Record in Scopus Google Scholar - Statistical Center of Iran
http://www.sci.org.ir/portal/faces/public/sci_en (3 January 2010, date last accessed)
Google Scholar - T. Morimoto, T. Nagao, K. Okazaki, et al.
Current status of breast cancer screening in the world
Breast Cancer, 16 (2009), pp. 2-9
CrossRef View Record in Scopus Google Scholar - K. Mohammad, S.M. Sadat Hashemi, F.K. Farahani
Age at natural menopause in Iran
Maturitas, 49 (2004), pp. 321-326
Article Download PDF View Record in Scopus Google Scholar - J.S. Mandelblatt, K.A. Cronin, S. Bailey, et al.
Effects of mammography screening under different screening schedules: model estimates of potential benefits and harms
Ann Intern Med, 151 (2009), pp. 738-747
CrossRef View Record in Scopus Google Scholar

